“Survival Depends on Their Permission”: Healthcare Under Armed Rule in Darfur

Medical staff try to revive a person wounded by shelling at Al-Nao Hospital in Omdurman, Sudan, September 5, 2025. The patient was later pronounced dead. Photo by Luke Dray.
Editor’s Note: I interviewed Sadeia Alrasheed on March 22, 2026, amid the continued destruction of Sudan’s healthcare system and the dismantling of the basic conditions necessary for life under the genocidal warfare carried out by the Rapid Support Forces. Since April 2023, Sudan has become one of the largest displacement crises in recent history, with 14 million forced from their homes and millions more pushed into hunger, medical abandonment, and conditions of permanent insecurity. The war, fought between the Sudanese Armed Forces under General Abdel Fattah al-Burhan and the Rapid Support Forces under Mohamed Hamdan Dagalo, known as Hemedti, has devastated civilian life across the country, but its violence has fallen especially heavily on Darfur, where the RSF and its Janjaweed lineage are inseparable from the earlier genocide of the 2000s. The numbers are staggering, but they only begin to describe the scale of destruction. Tens of millions of people in Sudan now require urgent humanitarian assistance. More than 24 million face acute food insecurity, and famine conditions have been identified in parts of the country, including El Fasher in North Darfur. Across the war’s first three years, Al Jazeera reported that one person was killed, on average, every 27 minutes. These figures mark Sudan not only as a humanitarian catastrophe, but as a sustained assault on the infrastructures that allow people to remain alive: hospitals, clinics, food systems, roads, refugee routes, maternal care, water, shelter, and the fragile local networks that continue to hold communities together when formal institutions collapse.
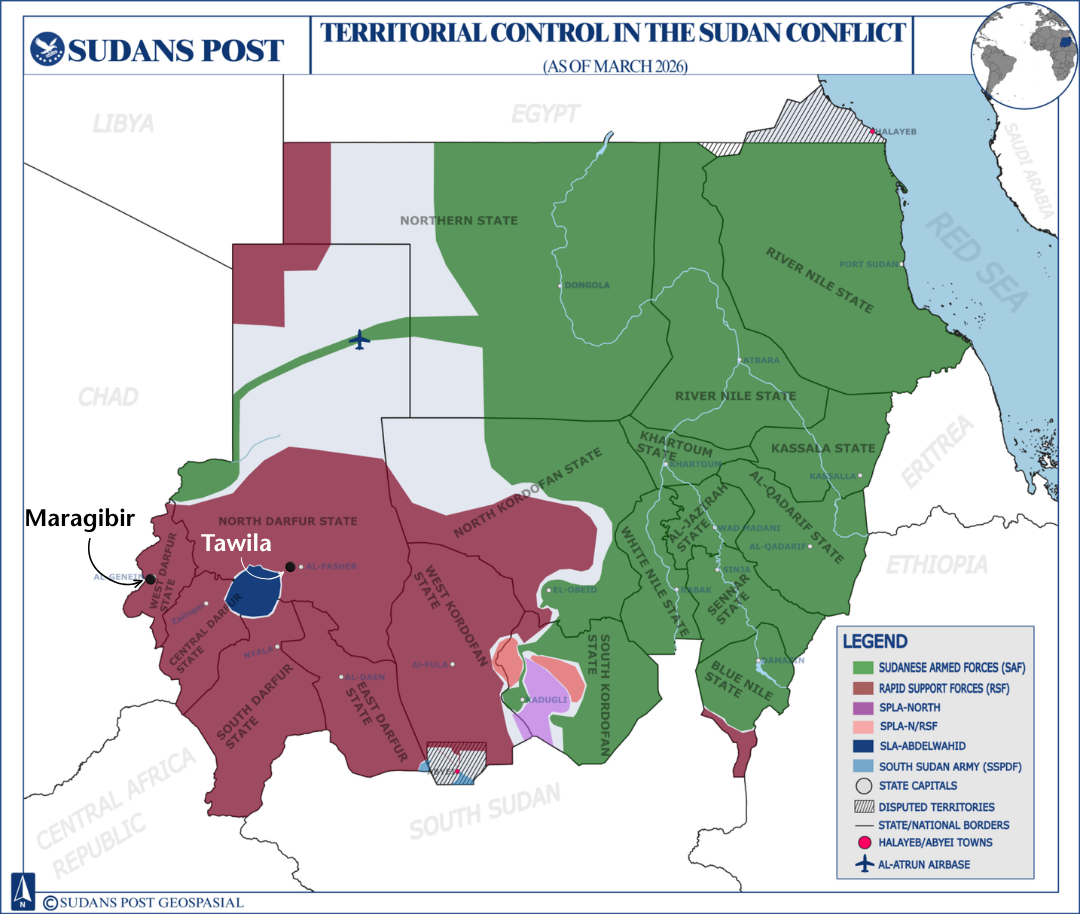
Sadeia Alrasheed is the Director of Hope and Haven, a Sudanese-led organization headquartered in Kampala, Uganda, with its main services operating in Adré refugee camp in Chad and a stationed presence in Tawila, North Darfur. Hope and Haven also supports emergency and community-based work in Bahri and Khartoum, Sennar, Al Jazirah, White Nile, and through partners across Sudan, Chad, Egypt, Ethiopia, and Uganda. Founded in June 2023, as large numbers of Sudanese families were forced to flee their homes toward Chad’s eastern border, the organization provides medical treatment, psychological trauma care, food and shelter support, and reconstruction materials for displaced people attempting to rebuild their lives. Its stated mission is to provide “a safe refuge and dignified life” for internally displaced people and refugees in Chad and across Sudan.
In this interview, Alrasheed speaks from the position of someone working inside the fractures of Sudan’s humanitarian and medical collapse. She describes Tawila, where more than a million displaced people live amid armed rule and where one of the only available health facilities was essentially a tent. She explains what it takes to move medication through merchant networks, checkpoints, cash economies, RSF-controlled territories, and routes from South Sudan and Chad. She details how doctors and humanitarian workers are coerced, threatened, detained, or forced to work under armed authority, and how survival itself becomes conditional on negotiation with those producing the violence.
Her testimony also moves beyond infrastructure into the body. She describes children whose skin, limbs, and growth bear the marks of famine, lack of vaccination, and maternal deprivation. She insists that discussions of children must begin with mothers, pregnancy, miscarriage, birth, and the collapse of prenatal and postnatal care. She speaks directly about sexual violence as a weapon of displacement, the stigma that keeps survivors from seeking treatment, the difficulty of documenting cases that official institutions refuse to recognize, and the impossible position of small Sudanese organizations expected to answer mass trauma with almost no funding.
Layered beneath the testimony of carnage and evisceration is a portrait of Sudanese survival under conditions designed to exhaust it. Alrasheed’s account shows how local organizations are forced to perform the work of hospitals, social services, trauma centers, supply chains, and emergency response systems at once. It also shows the cruelty of a global aid structure that demands impossible paperwork from people working with pen and paper, without stable internet, in areas where roads are unsafe and clinics themselves can become targets.
This interview has been transcribed and edited for clarity and length. It is published as part of an ongoing effort to document the medical and political realities of medicine and healthcare through the voices of those working closest to its devastation.

Courtesy of Hope and Haven
What does access to healthcare look like right now in Tawila, and how are displacement, armed control, and the collapse of formal institutions shaping what people are forced to rely on?
Let me draw out the situation by discussing the project we operate and are hoping to receive further help from the IOM. This project is for access to health by installing and renovating health clinics and facilities in Tawila.
Tawila, of course, is in North Darfur. This region is a place for more than a million displaced people. And when we talk about this place, you have to understand the politics. This place is mostly ruled by armed forces, not by the army. So in this area, we wanted to find health facilities to renovate. We found a single health facility. And basically, it was a tent.
This tent was supported by another organization, and this is the last month of their support. It is a very small tent. We even proposed to add seven more tents, just so it can become some sort of health facility, so it can absorb more people, more patients.
We are talking about an area where, when we counted the nearby camps, we calculated more than 40,000 people. And these people are only relying on traditional medicine. And traditional medicine means the fruits, the herbs, the things they can find. For example, if you have a broken bone, you go to someone who will fix it for you in the traditional way. They do not have access to modern viable health.
The Ministry of Health is not even functioning there. Even us, we had to get our certification and registration as an organization from the rulers of these areas. We would have to get our medical supplies either from areas where the RSF is ruling, or from a neighboring country.
To give you an example of how severe the situation is: when we tried to calculate how many children are going through malnutrition, we found that even grown-ups are suffering from malnutrition. We have people over eighteen who look like they are ten or twelve because of malnutrition.
So the conditions are absolutely getting worse and worse. Also it’s not just damaged facilities or sub par access to health. There is also the targeting of people who are working at the facilities, people whose main job is to heal who are now risking their lives working there, because there may be an invasion by the RSF.

Courtesy of Hope and Haven
What does it actually take to get medication into the clinics you support in North Darfur?
To answer your question, I want to make sure we understand that it depends on the area. This is part of the fragmentation I am talking about. For example, in Tawila, medication is available because local organizations like ours have built relationships with merchants and created a supply chain. Our network gets medication from South Sudan, and also through Chad, through Al Geneina. So yes, we have medication, but it is not consistent.
Let me explain. In some areas, especially those heavily ruled by the RSF, in order to get medication or even food parcels, you have to pay. And you have to pay a lot of money. You have to go and talk, negotiate with the ruling party, with the RSF, and show them that you are not related to any rival party. We tell them: let us help. Please let us help. This is good for you. This is good for the people you rule. We say this to show them that we are working in their benefit. And unfortunately, some people have had to collaborate with them, which is absurd. But what can you do? People are dying, literally.
In terms of getting medication, it is expensive, it takes a long time to reach, and it is not consistent. Sometimes it takes up to a week just to deliver some of it, let alone all of it. During the cholera outbreak, it took maybe a week or more to secure life-saving medication. I remember once it took us three to four weeks just to secure IV fluids for cholera, because people lose fluids during the illness, and they need those fluids just to survive that period. Compared to other regions, Tawila is costly, and everything takes a long time.
There is also risk. And I want to stress that risk is something we think about a lot. I remember one of our employees had cash with him, because that is how you interact and work with merchants in these areas. He was arrested by the RSF. They assumed he was related to the army. He was beaten, and they took the cash he had. We had to send an evacuation team to get him out of the area. So this shows you that it is risky even to carry cash to buy medication.
The whole process is expensive and very tricky. Some merchants will not accept Bankak, the app people use in Sudan to send money. They will say, no, we only take cash. So it is a very difficult process. It is not NGO-friendly, and it cannot be done easily by any outside party. There is a level of local knowledge here that only people from the area, or people already working inside these networks, can really understand and manage.
How does the RSF pressure hospitals, doctors, and health workers in the areas it controls?
One example of how the RSF governs healthcare is what happened in El-Fasher. When the RSF entered El-Fasher, my contacts on the ground said they killed many patients and doctors, and held others hostage. Some of those hostages were doctors, because the RSF needed them to treat their own wounded, their own soldiers.
There was also an element of propaganda in this. They needed to show the world that they were not just coming to invade, that life was continuing under them. I remember when a Sky News Arabia reporter went to the hospital and to these areas, and the image being shown was: look, things are okay, things are working. But this is propaganda. These people are not working freely. They are hostages.
At the same time, when I was trying to help people in Tawila, I was contacted by people who said they could get food inside El-Fasher. Immediately I understood what that meant. If you can get food inside El-Fasher, then you are working with the RSF, because there is no other way around it. You cannot enter the city without their approval. They said they were working in the emergency rooms, that they wanted to help people get food because they knew we had access to food. But because I am Sudanese, because I know the area and I know how these things work, I understood that they were connected to the RSF.
This is part of how the RSF pressures hospitals and doctors. They make survival conditional on their approval. They control who moves, who eats, who receives treatment, and who is allowed to work. But I do not judge people easily here. Some people are forced into impossible decisions. Some people become submissive because they are trying to survive, or trying to help others survive.
We experienced this ourselves in the Bahri emergency room when the area was under RSF control. We had to deal with RSF leaders. We had to go and speak to them and say: we need to work in this area. Please let us work. We are only helping our people. We are not related to the army or to any party.
So yes, the pressure is real. But it is complicated, because the RSF has control over life itself. They make survival dependent on their permission. And when you are trying to save lives under that kind of control, you are forced to negotiate with the very people creating the danger.
Is the violence against healthcare concentrated more heavily in Darfur, or are you seeing the same patterns across Sudan since the 2023 war?
If we are speaking historically, Darfur has carried this violence for a very long time. Since the wars of the 2000s, Darfur was targeted the most. The RSF came out of that history. They were there, they started there, and they did everything in that area. So Darfur is not new to this violence.
But if we are talking about the current war, the war that began in 2023, then we are not only talking about Darfur anymore. We are talking about many areas now suffering from the same things at the hands of the RSF. We are talking about Al-Jazirah State. We are talking about the Wad al-Noura massacre. We are talking about places where the RSF did the same kind of things, the same amount of violence, the same pattern.
The problem right now is that the country is split into safe and non safe zones with parts of northeast Sudan under the army and the government, where people have safe(er) lives. But Darfur is not safe. The war is still ongoing there. It is not a stable place. There are many armed forces, many parties involved.
In terms of types of attacks, we are not only talking about attacks from inside Sudan, as there have been attacks and movements coming from neighboring places, from Chad, from Libya, from other parts, even from Ethiopia (through South Sudan). All of this is what makes Darfur a hot zone. This is what makes it unsafe. This is what makes it targeted more.
Sometimes I feel that people who have the resources have just given up on Darfur. They stay in areas where it is safe and leave the locals to deal with their own suffering. They stay with the capital where the war is experienced much differently.
I often say that Sudan is not safe unless Darfur is safe. We are not safe unless this region is safe. Even in White Nile State (located just south of Khartoum) where Hope and Haven is also present, one of the communities we support was targeted near their area by the RSF. So we are not safe unless these areas are cleared, unless these areas are rid of the RSF. Until then, we are definitely not safe.
Courtesy of Sudans Post. Edited by Author
What pushes people to make the journey to Tawila, and what does that journey look like for displaced families trying to reach safety, food, or medical care?
The journey itself is costly. I do not think many people understand that displacement is not simple. It is not just that you leave. You have to think about it. You have to plan it. In order to leave your village, for example, you understand that you are leaving your livelihood. Many people are farmers. Many were already displaced since the 2000s and were already living in camps. After 2023, many of them are now displaced for the second or third time. So they know what displacement means. They know that the journey itself costs a lot.
You either go by car, and you pay a lot of money for people to move you. But they are not only moving you. They are promising you safety. They tell you: we will get you to the border. We have a route. We know where to go. If we meet the army or any militia, we will deal with them. We will pay them. We will take care of you. So the transport is not only transport. It is a whole promise of safety, and that promise is very expensive.
People who had to run recently, especially from El-Fasher during the RSF siege, had to make very difficult decisions. On the road, there is no water. There is no food. People are dying on the road, and they do not know where to go. Tawila is one of the areas that remains safer, and it is not ruled entirely by the RSF. There are also many organizations working there. So people come looking for treatment, or food, or safety. But they come with the risk that they may not reach at all.
Some people go on foot. They say, okay, tomorrow we will go to another place. So even when they come toward Tawila, it does not mean they will stay there because there is medical aid or food. There is always this need to move again, because no living condition is really tenable. It is a brutal displacement journey. It is not romantic. There is no lesson in it. It is full of anxiety. It is socially exhausting too, because you are constantly forced to deal with people, to negotiate, to be cheated, or even to cheat in order to reach where you need to go.
And on the road itself, it is ugly. Women give birth. People die. People are thirsty. People are carrying the injured. And even if you reach Tawila, it is not a haven. You reach a very long line of people. Not everything is available. People are trying to do something, any type of charity work. Small organizations are trying to help. But it is not like you will find food waiting for you, or a tent waiting for you. You may end up sleeping under a tree for days, waiting for a food organization to provide shelter or food.
And even with these organizations, there is a bureaucracy that is extremely backlogged. They need to log you. They need to register you. They need time. It is hard for us too, on the helping side. We want to help, but there is such a high number of people. It is untenable.
Beyond malnutrition, what kinds of illnesses and injuries are people coming to you with, and how has the war shaped both the need for healthcare and the danger faced by doctors themselves?
People are coming to us with other kinds of illnesses, of course. But we have to understand that these illnesses are connected. They are connected to injuries from war, to famine, to not having proper food for three years, to the collapse of education, to the breaking of families and social life, and to the healthcare sector itself being incapacitated.
And we are talking about Darfur, a region that has already been suffering for many years, especially since the genocide in the early 2000s. This is a place that already did not have basic infrastructure for medical care, or really for anything. Not even the infrastructure to maintain minimum life. Not even the conditions for a proper life. And now the war comes with all its severity.
Where the RSF is ruling, and where the RSF is going, there are attacks against the infrastructures that maintain life. This is a pattern we see across these areas. They target hospitals. They target doctors. I told you, we have a medical clinic just outside Marqabir. One of our doctors was working in Al Geneina Hospital when the RSF came into the area. They held her with others and forced her to work, to heal their soldiers. She managed to escape later and went to Adré, Chad, just across the border.
So as a medical practitioner, you are either targeted by killing, or you are forced to work with the RSF. And these are horrible conditions. You are always thinking that you may not survive, either because of the living conditions, or because you may be killed. One day they may decide you are not valuable anymore. They may erase you because you are evidence of what they did.
So yes, health is being weaponized, and healthcare workers are being criminalized. But more than that, we are treated as useful only until we are not useful anymore. Humanitarian workers and doctors can be erased once they are no longer valuable. And this affects us. It affects our families. It affects everyone around us.

Courtesy of Hope and Haven
What are you seeing in children’s bodies now, beyond hunger itself?
You are right to ask about starvation, and especially about the thinness of children. But I want us to think beyond the idea of being skinny in the Western sense. In Sudan, people are often skinny because of the way food, daily life, and mobility are shaped. People from Darfur and South Sudan, for example, are often tall and skinny. They have this bright skin. I do not mean light skin in the traditional sense. I mean skin that is glowing, bright from the sun, from working on farms, from daily life.
But the children today are different. The bodies of children being born now, especially over the last year and through these years of violence, are changing. You can see the violence of the country in the body itself. And I think it starts with the mother. The mothers themselves are not healthy. In one camp in North Darfur, I think in 2024, all the pregnant women in that specific camp miscarried. All of them. They had no access to medical care, no proper food. So when the mothers are unhealthy, when their bodies are weakening, of course the children are also born weak.
Many children are not getting proper vaccination. Many develop skin conditions because they are so thin. My staff tell me that when they measure them, they measure the arm to see how severe the malnutrition is. The reports come back with general weakness. The skin itself is thin. That is the level of malnutrition. The skin itself is thin. So imagine what the rest of the body is like. Imagine what the bones, the muscles, the whole body is going through.
We are seeing pictures and scans of children whose heads look larger than their bodies. These problems are connected to many things: lack of food, lack of vaccination, lack of treatment, the condition of the mother, the war itself. It is frustrating because we have been telling people for a long time that this is happening, and the trend is becoming more and more alarming.
Even the birth conditions are terrible. There is no sterilization. There is nothing. And even if the child lives, many children come to us needing surgeries, procedures, and care just to allow them to develop. Many have hernias, tumors, or masses in the abdomen, in the head, or in sensitive areas. I do not know where all of these masses are coming from. Maybe from the war itself, maybe from scarcity, maybe from the conditions there. But many children are not healthy. Most of them need treatment.
This has become very noticeable after the war, especially in this period, because many children are reaching us only when they already need surgery. And then I think about those who never reach us. What would the number be? It is daunting. It keeps me up at night.
You also mentioned violence against women and girls. How is this violence being used in Darfur and in other areas of Sudan, and what does it do to families and communities?
The violence against women and girls precedes this war. Even before the war of 2003, this kind of violence was used by militias as a weapon. In Sudan, it has been one of the main weapons used to destroy people and tribes, because the aim is to force them to leave the area. It creates enough fear, shame, and anxiety that people feel they cannot stay. When your family is attacked in this way, you are afraid. You leave. You take your family and go, because the violence does not only harm the person. It scars the family, and it scars the whole community.
There is also the way these militias perceive women and girls from these communities. They look at them as slaves. And when we speak about this violence, we are not only talking about young women. We are talking about children as young as 3, elderly women as old as 70. In Al Jazirah, for example, when they entered, they attacked married women more than unmarried women. Why? Because it creates more pressure. It breaks the family. It forces people to leave the area.
In Darfur, because this has been happening since 2003, there is more awareness. People know that this is a weapon used against them. There has also been more access to organizations that speak with survivors, explain the protocols, and help them understand how to seek protection and survive after these attacks. But when this violence became more prominent in places like Al Jazirah and Khartoum, people were not prepared in the same way. Now we are seeing children born from these assaults. We are seeing women and families who cannot get the help they need because they do not want to speak about what happened. There is a blockage in our ability to help them because silence becomes part of survival. Some prefer to stay silent rather than speak about it.
So when we talk about the numbers of sexual violence cases in Sudan, the real number is much higher than what is reported. And because many people are not able to speak or access care, we are also seeing the spread of hepatitis and other diseases. These cases also involve men. It is not only women.
The aim is to break the will of people and force them to leave their homes. There is also a strange racial logic to it. Some perpetrators say they are “improving the lineage” through this violence. In Wad al-Noura, for example, men went into these areas and told women that they would become their husbands, that they would become their men, that these women now belonged to them. This is a form of slavery.

Courtesy of REUTERS/El Tayeb Siddig
When survivors of sexual violence reach your organization, what kind of care can you actually provide, and what are the limits of that care?
To understand this, you have to understand how our work is organized. In Chad, we have a center for psychological trauma treatment. It receives survivors of sexual violence, and also survivors of war violence. Some of these cases began reaching us in 2023, after people entered Chad in June. But because we are Sudanese working in Chad, these cases come through medical access. MSF is the organization that registers them and works under the medical treatment protocol. There is a protocol for rape cases. After the survivor receives medical attention, then the case can come to us. What we provide is the psychological and therapeutic part. We cannot intervene in the medical part, even if we have specialists, because in the end we are Sudanese working in a foreign country.
Inside Sudan, the work was different. We worked through the Bahri emergency room, and we had rape kits. Usually, the report would come to us through people. Someone would know of a case and tell the survivor: please, these are the numbers, call them. Then she would call us, and we would try to reach her. But at that time, the roads were unsafe, so even delivering the rape kit had to happen through people. And the rape kit itself only works if it is taken within the first three days, unfortunately. Many women are assaulted and then forced to leave immediately, so they do not have access to the kit in time. After that, what we can do is work with them psychologically.
How are these cases documented, and why are the numbers always lower than what actually happened?
There is an existing registration system. Some women choose that it is okay, for example, for lawyers to register their case: that I was raped on this day, by this number of people, in this place. But the reality is that, with all the systems and statistics that exist, many choose not to come forward. There is also a prioritization of which statistics get highlighted. We do have statistics, but unfortunately, in the system we live in, they are not considered “official.” We are not the Ministry of Health, for example. We are not affiliated with the UN or with an INGO. So there are statistics specific to small organizations like us, and to emergency rooms, but they are not treated as accurate in the sense of being official.
And as I am telling you, the number is very large. I personally know people who have been assaulted. I will give you one recent example. One man was trying to protect his family, and he was injured. He refused for us, as an organization, to provide him treatment through sending his data and information, because he did not want to mention the reason it happened. And the reason was that he was defending his daughters from being assaulted. Unfortunately, his wife was raped. His daughter survived, but his wife was raped, and no protocol was done for her. Most people choose silence.
Because of this, there are many birth cases in the community itself. Some are accepted. Some, unfortunately, are abandoned. There are children now without support because of this, many neglected children. In the areas where we work, we do not have access to intervene in this issue, or it is not allowed for us. In other areas, like Bahri, where the Ministry of Health is working, we are not allowed to work on these things. But in Darfur and these areas, we are also restricted by social stigma, by access, and again by funding. We are so limited in what we can do.
What would it cost to provide this care properly, and what are small organizations like yours struggling with month to month?
We could do many things. We have the knowledge. We have the personnel. We have the staff. We have people who can work, people who have the networks, and people who have the capacity to survive in these areas because many of them are going through the system themselves. They are going through this oppression too. The only place where we lack capacity is fundraising. Funding. We do not have enough funds. And this is the issue that many small organizations go through.
For example, in Tawila, one of our medical facilities costs around $15,000 a month. This is only to see between 50 and 75 patients daily. And even this facility does not treat everything. We treat malaria cases, cholera cases, and we do minor surgeries, like cuts and small injuries. We also have a laboratory. This alone costs $15,000 a month.
As for the trauma center, it may cost around $5,000 a month for up to 56 patients or cases per month. We provide treatment for three months. This includes psychological rehabilitation. Within that psychological rehabilitation, there are motivational programs and reintegration programs, so that women can work again, stand again. There is also a safe space for children. So this is what medical care means for us, according to our intervention. We try to build the kind of infrastructure that allows our patients to leave not only treated, but able to become active members of society again, able to resist.
But we struggle so hard just to survive month by month. We have fundraising programs online, but of course that is not reliable. It goes up and down. If another disaster happens somewhere else in the world, the focus shifts immediately away from Sudan. And Sudan has not been getting the attention it should. So sometimes we have had to stop work. We are forced to wait, because people cannot continue to work without income.
There are also organizations that try to support us, but sometimes they support us for only one month, and they ask for very complicated things. The bureaucracy and paperwork required just to support us for one month is untenable. For example, we have support from one of the largest organizations, one that supports gender programs and rehabilitation funds. They give us support, but they give me way too much paperwork to fill out. They do not only need our simple financial reports. They need everything down to the dot.
But they do not understand that we have people on the ground who write with paper and pen. They do not have technology. They do not have access to internet. So it becomes another layer of inaccessibility.